

10 epilepsy facts
In this article we will describe 10 medical revision notes about epilepsy.
Key Points
- Epilepsy is a neurological disorder characterized by recurrent, unprovoked seizures resulting from abnormal electrical activity in the brain.
- It affects people of all ages, with a variety of causes, ranging from genetic factors to structural brain abnormalities.
- Management involves accurate diagnosis, appropriate anti-epileptic medication (AED) selection, and addressing lifestyle factors.
- Early diagnosis and tailored treatment are essential to improve patient outcomes and quality of life.
- Education and support for patients and families are crucial aspects of care.
1. Definition
- Epilepsy is a chronic neurological disorder defined by the occurrence of two or more unprovoked seizures, separated by at least 24 hours
- Seizures are transient episodes of abnormal, excessive, or synchronous neuronal activity in the brain
- Epilepsy can be classified into focal (partial), generalized, and unknown onset seizures, based on the initial area of brain activity.
2. Epidemiology
- Prevalence: Epilepsy affects approximately 1 in 100 people in the UK, with around 600,000 people living with the condition. It is one of the most common neurological disorders globally.
- Incidence: There are about 32,000 new cases diagnosed annually in the UK.
- Age Distribution: The incidence of epilepsy is highest in early childhood and older adults, with peaks in those under 10 and over 65 years of age.
- Gender: It affects males and females equally, though certain epilepsy syndromes may have a gender predilection.
3. Risk factors
- Family history of epilepsy or febrile seizures
- Previous central nervous system (CNS) infections (e.g., meningitis, encephalitis)
- History of head trauma
- Prenatal or perinatal factors (e.g., birth asphyxia, low birth weight)
- Stroke or cerebrovascular disease
- Neurodevelopmental disorders (e.g., cerebral palsy, autism)
- Brain tumors or lesions
4. Causes
Genetic
- Idiopathic Epilepsy: Often has a genetic basis without identifiable structural brain abnormalities.
- Genetic Epilepsy Syndromes: Conditions such as Dravet syndrome, childhood absence epilepsy, and juvenile myoclonic epilepsy have specific genetic mutations.
Structural
- Brain Injury: Trauma, surgery, or cerebrovascular incidents can cause scarring that leads to seizures.
- CNS Infections: Meningitis, encephalitis, or abscesses can lead to epilepsy.
- Tumors: Brain tumors may cause seizures, often presenting as focal seizures.
- Neurodevelopmental Abnormalities: Congenital conditions such as cortical dysplasia and tuberous sclerosis.
- Metabolic Disorders: Conditions like hypoglycemia, hyponatremia, and mitochondrial diseases.
5. Symptoms
- Seizures: Symptoms vary depending on the type of seizure.
- Focal Seizures: May involve motor, sensory, autonomic, or psychic symptoms without loss of awareness (simple partial) or with altered awareness (complex partial).
- Generalized Seizures: Include absence seizures, tonic-clonic, myoclonic, and atonic seizures. These involve both hemispheres of the brain and often cause loss of consciousness.
- Aura: Some patients experience a sensory warning (aura) before a seizure, which may include visual disturbances, strange smells, or a feeling of déjà vu.
- Postictal State: Confusion, fatigue, or headache following a seizure.
Note. What are the different types of epilepsy? There are over 50 different types of seizures and epilepsy, and a person can have more than one type. Seizures can be very different, depending on where in the brain they are happening. Some people remain aware throughout, while others can lose consciousness.
Seizures are generally divided into two main types: focal seizures and generalised seizures.
Focal seizures – only affect one part of the brain. People can experience focal seizures with full awareness or limited awareness
Generalised seizures – usually affect the whole of the brain and people will cause loss of consciousness, even if for just a fraction of a second.
What is a seizure?
A seizure is a sign of temporary disruption to brain function, caused by excessive electrical activity.
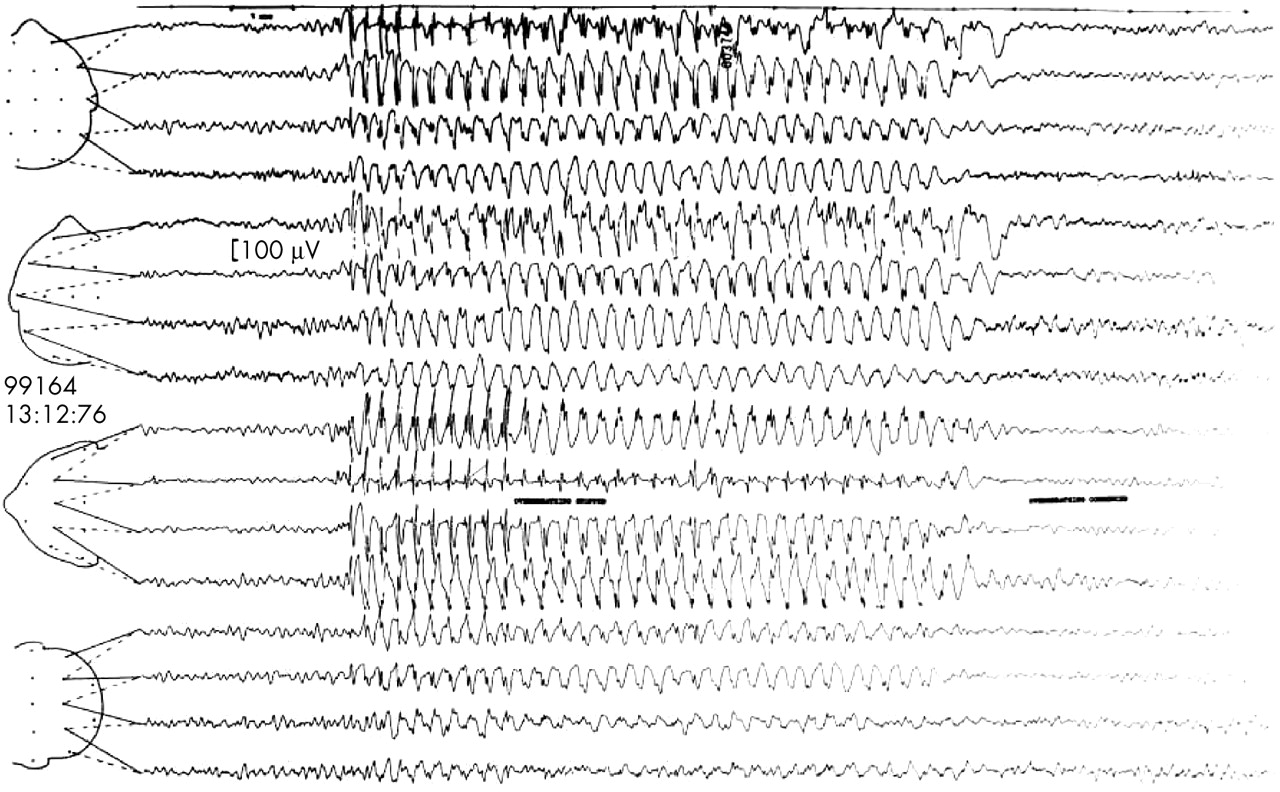
An EEG (electro-encephalograph) of the brain as a seizure starts
6. Diagnosis
Diagnostic criteria
- At least two unprovoked seizures occurring more than 24 hours apart, or one unprovoked seizure with a high risk of recurrence (e.g., due to an identified structural brain abnormality).
Investigation
- Clinical History: Detailed seizure history (including triggers, frequency, and duration) is crucial for diagnosis. Family history and any potential risk factors should also be assessed.
- Electroencephalogram (EEG): To detect abnormal brain electrical activity. Interictal spikes or abnormal waveforms may support the diagnosis.
- Neuroimaging: MRI is the preferred imaging modality to identify structural causes of epilepsy, such as tumors, vascular malformations, or cortical dysplasia. CT scans may be used in emergencies.
- Blood Tests: To exclude metabolic or systemic causes, including glucose, electrolytes, liver and renal function, and toxicology screens.
Differential diagnosis
- Syncope: Often mistaken for seizures, but usually involves brief loss of consciousness with rapid recovery.
- Psychogenic Non-Epileptic Seizures (PNES): Often resemble epileptic seizures but are psychological in origin.
- Migraine: May present with visual disturbances or aura that can mimic a focal seizure.
- Transient Ischemic Attacks (TIA): Can cause transient neurological symptoms, sometimes mimicking focal seizures.
- Movement Disorders: Conditions such as tics, myoclonus, and tremors may be confused with epilepsy.
7. Treatment
Pharmacological
- Anti-Epileptic Drugs (AEDs): Choice of medication depends on seizure type and patient-specific factors (e.g., age, coexisting conditions). Common AEDs include:
- Carbamazepine: Often used for focal seizures.
- Sodium Valproate: Effective for generalized seizures, though contraindicated in women of childbearing age unless other options are unsuitable.
- Lamotrigine: Broad-spectrum AED, suitable for focal and generalized seizures.
- Levetiracetam: Increasingly used due to its favorable side effect profile.
- Drug Titration: Start with a single AED and titrate dose based on efficacy and tolerability. If seizures persist, consider combination therapy.
Non-pharmacological
- Surgery: Considered for patients with drug-resistant epilepsy, particularly when a resectable brain lesion is identified.
- Vagus Nerve Stimulation (VNS): An option for drug-resistant epilepsy when surgery is not feasible.
- Ketogenic Diet: May be effective, particularly in children with refractory epilepsy.
- Lifestyle Modifications: Adequate sleep, stress reduction, and avoiding known seizure triggers.
8. Complications
- Injury: Risk of falls, burns, and accidents during seizures.
- Status Epilepticus: A medical emergency defined as a seizure lasting more than 5 minutes or repeated seizures without recovery between them.
- Psychosocial Impact: Anxiety, depression, social isolation, and stigma are common in epilepsy patients (see below)
- Sudden Unexpected Death in Epilepsy (SUDEP): Rare but significant risk, particularly in patients with poorly controlled tonic-clonic seizures.
9. Prognosis
- General Prognosis: Around 70% of patients with epilepsy achieve remission with appropriate treatment. Seizure freedom for more than 2 years may prompt consideration of medication withdrawal, though this should be approached cautiously.
- Factors Influencing Prognosis: Etiology, age of onset, seizure type, response to AEDs, and adherence to treatment play a role. Patients with idiopathic epilepsy tend to have a better prognosis than those with structural causes.
10. Prevention
- Primary Prevention: Minimizing risk factors where possible, such as preventing head injuries, controlling prenatal risk factors, and managing comorbidities (e.g., hypertension to reduce stroke risk).
- Secondary Prevention: Early identification and treatment of epilepsy to prevent complications and improve quality of life.
- Patient Education: Educate patients on adherence to AEDs, avoiding triggers, and safety measures (e.g., not swimming alone, using protective headgear if at risk of falls).
Consequences of a diagnosis of epilepsy
A diagnosis of epilepsy can have life-changing consequences. These can include the loss of a driving licence, reduced independence, and disruption to employment. It can also affect someone’s education and employment prospects, and lead to an increased degree of social isolation and depression.
Suggested terminology for people with epilepsy
- People do not want to be defined by their condition. So please do not call someone with epilepsy, an ‘epileptic’ – or for that matter do not use phrases like ‘alcoholic’ or ‘diabetic’. Doctors don’t do adverbs. It is important to see the person and not the medical condition. It is more helpful to say ‘a person with epilepsy’
- The term ‘seizure’ or ‘epileptic seizure’ are preferred to the phrase ‘fit’
- A ‘victim’ or ‘sufferer’ implies someone is helpless. This is not helpful language when describing people with epilepsy, or any chronic disease. It’s better to say a ‘person is affected by or living with epilepsy’
- Grand mal seizures are now called tonic-clonic seizures
- Petit mal seizures are now called absence seizures.
Summary
We have described 10 medical revision notes on epilepsy. We hope you understand it better now.
Top Tip
Epilepsy is a syndrome with many types, sub-types and causes. It’s important to classify and treat it carefully. Think about the language you use when dealing with patients with the condition.
Other resource
MyHSN epilepsy podcast (2024) – 7 min, 46 sec
