

Chest x-ray interpretation: 7 steps

This is a normal chest x-ray.
In this article, we will describe how to interpret a chest x-ray in 7 steps (ABCDEFG), after correctly identifying the patient, and describing the type of x-ray.
You need to know your anatomy.

Firstly .. identification, and what type of chest x-ray is it?
Identification (ID)
- ID: verify the patient’s name, date of birth, and the date the x-ray was taken to ensure you are examining the correct image
- Orientation: is the x-ray oriented correctly? Check that the x-ray is displayed with the patient’s left side on the correct side of the image
- Artefacts: any artefacts obscuring the image (e.g. jewellery)?
- Man or woman: look for breast shadows; any (i.e. man/woman)? 2 breasts?
Type of x-ray
- Type: posterior-anterior (PA), anterior-posterior (AP), lateral? Combination?
Note. PA is the common view. The x-ray plate is touching the patients chest, with the x-rays coming from behind (hence posterior).

After this .. 7 steps (ABCDEFG). Here goes.
1. A – Assessment of quality – is it good quality?
Does it RIP? ..
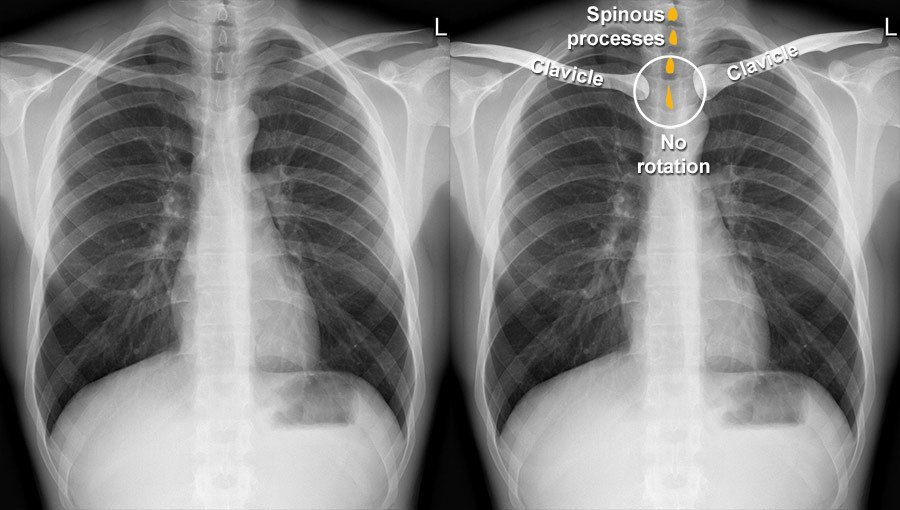
- Rotation – trachea should be equidistant between the clavicular heads, i.e. centred in the chest
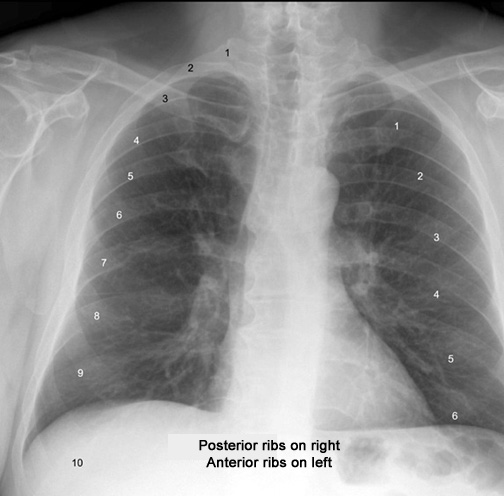
- Inspiration – 6 anterior (and 10 posterior) ribs should be visible if fully inspired
- Penetration – the spine should be just transparent through the heart.
2. B – Bones – any abnormalities?
- Bones: assess the ribs, spine, and clavicles for fractures, lesions, or other abnormalities.
Note. Soft tissue (see below) are often done here, so you don’t forget it.
3. C – Cardiac and mediastinum – are they normal?
- Assess the heart size and shape. The cardiothoracic ratio (CTR) should be <50% (<60% on APs; not reliable to assess heart size)
- Evaluate the mediastinum: for widening or masses
- Check for: calcification, and prosthetic valves.
4. D – Diaphragm – is it normal?
And what about above and below it?
- Above: any fluid in costodiaphragmatic angles (pleural effusion?)? The angles should be sharp
- Diaphragm: check the hemidiaphragms for position (the right is slightly higher than the left due to the liver) and shape; may be flattened bilaterally in chronic asthma or emphysema, or unilaterally in case of tension pneumothorax or foreign body aspiration)
- Below: look below the diaphragm for free gas (perforated viscus?).
5. E – Extrathoracic soft tissue – any shadows or densities?
- These can be normal or indicative of various conditions, including obesity, foreign bodies, or subtle signs of disease.
6. F – Fields (lungs) and foreign bodies – what do they look like?
- Lung fields:
- Check for lungs masses, consolidation (+/- air bronchograms), and pneumothoraces
- Compare R to L, in upper, middle and lower zones
- Fissures: check for them
- Vascular markings: vessels should taper and should be almost invisible at the lung periphery
- Foreign bodies (check for): e.g. ET or NG tubes, pacemakers or pacemaker leads, central venous pressure (CVP) lines etc. Comment on previous surgery, e.g. cholecystectomy clips, sternotomy wires.
7. G – Gastric bubble – is it present?
- The gastric bubble should be seen clearly and not displaced.
- Apices (TB?)
- Peripheral lung margins (rib fractures?)
- Hilar, retrocardiac, and costodiaphragmatic angles.
Finally finally .. right test – is it right investigation for this patient?
- Right test? – e.g. the CXR is usually normal in someone with an MI or PE.
By answering these questions, you will have a systematic approach to reading a chest x-ray.
How to present a chest x-ray
“This is a PA chest x-ray of Mr/Mrs X/Y. The heart is of normal size with a CTR of under 0,5. The lungs are clear. It is normal”
Or
“This is an AP chest x-ray. I therefore cannot comment on the heart size. There is increased shadowing in the R lower zone. The most likely diagnosis is pneumonia, but the differential includes pulmonary haemorrhage and embolism”.
Summary
We have described how to interpret a chest x-ray in 7 steps (ABCDEFG). We hope it has been helpful.
Determining the quality
- Rotation: compare the positions of the left and right medial clavicular joints to the spinous processes. There should be an equal gap on each side, as shown in the following diagram
- Inspiration: count the ribs visible in the lung fields. There should be 10 posterior (8 is minimum) and 6 anterior ribs
- Penetration: the vertebrae behind the heart are just visible.
MNEMONIC – RIP
Other resource
